Long COVID is a term used to describe patients with returning or sustained symptoms following a SARS-CoV-2 infection. Physicians and researchers have described numerous post COVID-19 complications, including cardiovascular, coagulation and hematologic, gastrointestinal, kidney, mental health, metabolic, musculoskeletal and neurologic disorders [1]. The CDC recently published findings that 1 in every 5 COVID-19 survivors “experienced at least one incident condition that might be attributed to previous COVID-19” [2].
The risk factors for developing long COVID-19 are being studied within the United States and across the world [3, 4, 5]. We conducted independent research to learn more about 1) who is being diagnosed with long COVID from a large population all based in the United States and 2) if those diagnosed had been hospitalized in the first 30 days following an initial COVID-19 infection?
Methods:
We looked at a subset of the Truveta dataset through June 17, 2022. We identified people who had received a diagnostic code associated with long COVID in their electronic health record. Codes included were ICD10CM U09.9 (Post COVID-19 condition, unspecified) and SNOMED CT 1119303003 (Post-acute COVID-19).
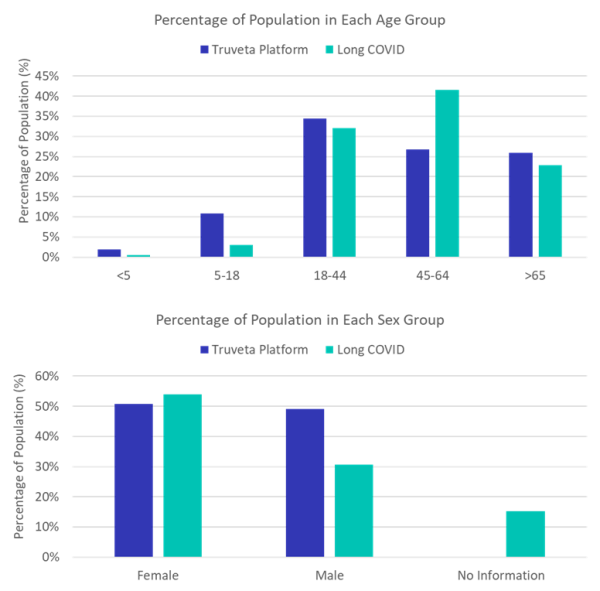
We then stratified this population by age and sex. Within each demographic group we compared the percentage of the population who was diagnosed with long COVID to the overall Truveta Platform demographics.
We also investigated the percentage of population who had a positive COVID-19 PCR test or COVID-19 diagnosis prior to the long COVID diagnosis and was subsequently hospitalized within 30 days of the first indication of COVID-19.
Results:
Within this subset of our data, we identified over 30,000 patients diagnosed with long COVID. The demographic data of the patients diagnosed with long COVID as well as the demographic distributions within the Truveta Platform are shown in the graphs below.
The Truveta data contains de-identified health records. In the process of de-identification, variables (such as demographics) are concealed to protect a person’s identity. The unknowns in this report either demonstrate missing values in the EHR or concealed data to ensure a person is not able to be re-identified [6].
Discussion:
These data show long COVID was diagnosed across age and sex groups. In our data females were diagnosed at a higher rate (54%) than the percentage of the population they make up. Females are also nearly two times more likely to be diagnosed with long COVID than males.
We also see that while those aged 45-64 make up 27% of the population in our data, they comprise 42% of long COVID diagnoses, while those 18-44 make up 32% diagnoses and those over 65 years old account for 23% of diagnoses.
We found that 22.4% of the population diagnosed with long COVID was hospitalized within 30 days of the first COVID-19 indication.
There are a few limitations with the methods presented in this report. First, we compared to the demographics of the long COVID population to the population within the Truveta Platform. We assumed physicians across our health systems are using the diagnostic codes associated with long COVID. As there have been challenges with defining long COVID, further work is necessary to potentially refine these definitions. Further, there may be heterogeneity in how long COVID is diagnosed, which would affect these results.
Conclusion:
This report helps give a descriptive analysis to the population diagnosed with long COVID. These data highlight the ability for researchers using Truveta data to investigate near real-time trends in diagnoses and treatments to better understand the population at risk. With this patient population, researchers are able to dig deeper to find trends in these patients with the hope of finding similarities, which may enable research toward better treatment pathways.
These are preliminary research findings and not peer reviewed. Data are constantly changing and updating. These findings are consistent with data from June 17, 2022.
Citations:
[1] Al-Aly, Ziyad, Benjamin Bowe, and Yan Xie. “Long COVID after breakthrough SARS-CoV-2 infection.” Nature Medicine (2022): 1-7.
[2] Bull-Otterson L, Baca S, Saydah S, et al. Post–COVID Conditions Among Adult COVID-19 Survivors Aged 18–64 and ≥65 Years — United States, March 2020–November 2021. MMWR Morb Mortal Wkly Rep 2022;71:713–717. DOI: http://dx.doi.org/10.15585/mmwr.mm7121e1.
[3] Yong, Shin Jie. “Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments.” Infectious diseases 53.10 (2021): 737-754.
[4] Sudre, Carole H., et al. “Attributes and predictors of long COVID.” Nature medicine 27.4 (2021): 626-631.
[5] Davis, Hannah E., et al. “Characterizing long COVID in an international cohort: 7 months of symptoms and their impact.” EClinicalMedicine 38 (2021): 101019.
[6] Truveta. Our Approach to protecting Patient Privacy. Spring 2022. Truveta’s Approach to Patient Privacy.